Robotic Assisted Laparoscopic Prostatectomy (RALP) is now the most common surgical treatment for prostate cancer in the United States. Over 80% of radical prostatectomies are done this way. In appropriate hands the da Vinci Robotic Assisted Laparoscopic Radical Prosatatctomy consistantly provides excellent results particularly in relation to cancer cure, continence and potency.
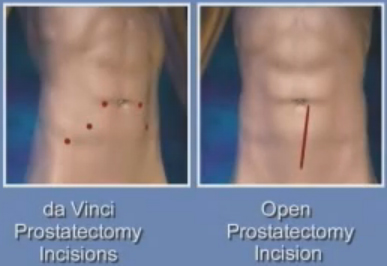
It is performed though 5 or 6 small keyhole incisions in the abdomen for the introduction of the laparoscopic ports. The traditional open method involves a larger incision from below the umbilicus to the pubic bone. The abdomen is inflated with carbon dioxide to create a surgical working space.
(fig showing large cut vs 5 small cuts)
The procedure was first performed around 10 years ago and had become increasingly popular due to the benefits inherent in the technological advances.
These benefits are derived from:
Improved visualisation with enhanced high def (1080) imaging with 10x magnification and 3D vision
Motion scaling with tremor filtration that eliminate tiny uncontrollable movement in the surgeons hand.
An ergonomic way of performing the procedure as the surgeon sits at a console and utilizes the enhanced visualisations and controls.
The small incisions of the laparoscopic approach allow for quicker return to normal activity, shorter hospitalization (most patients stay only overnight), less blood loss and transfusions and reduced pain.
It is clearly established that the use of the robotic approach is not responsible for the outcome but the surgeon at the console. Thus an average surgeon will perform an average robotic operation just as an average open surgeon will perform an average open procedure.
Why Robotic Prostatectomy
In the past the traditional open method was performed via a large midline abdominal incision and this was associated with significant morbidity, high volumes of blood loss requiring transfusions, significant pain and long hospital stays. This resulted in high risk of urinary incontinence and erectile dysfunction. Advances in technique and a better understanding of the anatomy have led to much better chances of cure and much less risk for incontinence and erectile dysfunction.
The robotic assisted laparoscopic prostatectomy is the latest and most technologically advanced change in the surgical treatment of prostate cancer.
How can the robotic approach improve the results
Due to the above mentioned improvements with access in particular fine, accurate and tremor free movements, enhanced high definition 3D vision the vital anatomy of the small blood vessels and nerves and surgical planes can potentially be recognised more readily and left undamaged resulting in less post-operative incontinence and erectile dysfunction.
The smaller incisions result in less pain, a faster recovery and return to normal activities.
What can I expect after surgery
Most patients would stay overnight and leave hospital the following morning. The rest may stay a day or two. On discharge the pain should be minimal and usually regular paracetomol would suffice.
All patients will go home with a catheter and a leg bag. The staff ensure all patients are very comfortable with this equipment before they leave the hospital. Both written and verbal instructions are given.
Results
It is very important to understand that da Vinci robot like any other instrument is just a tool of the surgeon and its use does not mandate good results. A good surgeon will achieve good results no matter which technique is used. However if a good surgeon utilises the technological advances of the robot then a better operation should occur.
Dr Vass has performed over 600 laparoscopic radical prostatectomies and has helped establish this procedure in Australia. His outcomes with the da Vinci robot have been excellent.
When most surgeons take up this new technology there is a period of time during which the surgeon learns and refines the procedure called the 'learning curve'. The exact number of cases after the surgeon is competent varies with the skill of the surgeon. Most units in the world report that an initial time taken to perform the operation is between six - ten hours. Dr. Vass's first case was below 3.5 hours and no case since then has taken over 3 hours.
Dr. Vass's current results:
PT2 positive margin rate below 3.5%. Only focal positive margins have been reported no extensive.
Operative times 1.5 – 2.5 hours
Bed stay >50% home day 1 (overnight stay only)
Average blood loss <100ml (no blood transfusion given)